Often there are two types of people that enter an outpatient physical therapy clinic following a surgery. Person number 1 is the individual who is excited to start because they want to do as much as they can with the idea that “more is better.” They are consistently calling to make an appointment for the next open slot at the clinic to get in as soon as possible. This patient is seen doing extra exercise repetitions, performs their home exercises consistently, and often begins to walk the line with their post-surgical precautions earlier than their surgeon recommended.
Person number 2 is the individual who is apprehensive and may be even nervous to begin physical therapy. They may wait longer than recommended to begin their physical therapy. This individual does not want to injure themselves further, and they want to avoid feeling more pain than they need to. This individual may be less likely to do their exercises regularly for fear of “messing up” the surgeon’s excellent work.
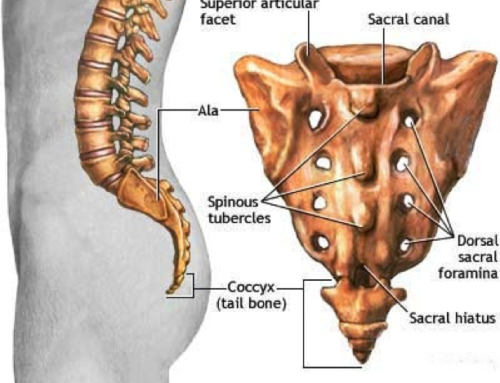
Now, you may not fall perfectly into one of these categories, but you get the idea. The question is how soon should you begin rehabilitation following a spinal fusion. Surprisingly, person number 2 may be on the right track with how post fusion rehab should be approached, initially.
In a multi-center, randomized controlled trial, 82 patients who underwent a spinal fusion were randomly assigned to two groups. One group began rehab at 6 weeks post surgery, and the second group began at 12 weeks post surgery. Outcomes of pain level and disability were assessed throughout rehab and up to 1 year following the start of the study. Results found those who began rehabilitation 12 weeks following surgery had better outcomes on measures of pain and disability. Therefore, delaying the start of physical therapy after a spinal fusion may be more beneficial when it comes to measures of pain and disability.
However, there was no difference between groups in their ability to return to work when compared at the 1 year follow up period.
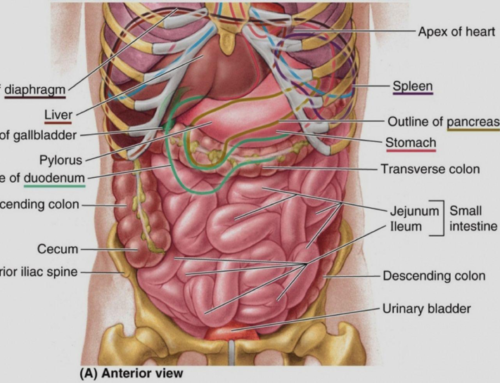
Tissues go through 3 phases of healing: acute inflammation, cell regeneration, and cell remodeling. The body is smart, so following a surgery, it is important to let the stages of healing occur with proper protection to the area. Initially, the body will be inflamed as healing factors are brought to the area. Cell regeneration begins in soft tissue approximately 2 days following an acute injury and can continue up to 8 weeks following an injury. This is why the surgeon and your therapist will stress the importance of following any post-surgical precautions. Tissue cell remodeling occurs as soon as 6 weeks and for up to a year following a spinal surgery. Therefore, ensuring you have adequate guidance as you progress your exercise program can help any detriments to returning to optimal function.
Often times as a therapist, I find myself reminding post-surgical patients to let the body do what it does. HEAL. The body knows how to heal and we are built with a system of cell communication that allows that to happen efficiently. Some of the best things you can do after a surgery to facilitate this process include eating a healthy diet, drinking plenty of water and getting quality sleep to optimize the healing process. Prior to undergoing a surgery, make a plan with your physician on the best timing to begin outpatient physical therapy. Keep in mind, the research presented above focuses on spinal fusion surgery, therefore, this approach cannot be extrapolated to other orthopedic surgeries. For example, many individuals are encouraged to get up and walk after a total hip replacement and this remains a common practice today for optimal rehab. Following a spinal fusion, your physical therapist will perform an evaluation and determine a course of action to get you back to performing at optimal functioning. Post-surgical rehabilitation for spinal fusion is a common condition seen here at John Goetze Physical Therapy. Make a plan with your surgeon and physical therapist today to ensure you are on the track to recovery after you leave the surgical table.
Spine (Phila Pa 1976). 2012 Oct 1;37(21):1803-9
—
Kathryn Wood PT, DPT, CIDN